The following white paper compares the calibrated flow signal from Nox Medical's RIP belts to a gold standard pneumotach measurement.
The white paper shows that the calibrated RIP flow signal has very high correlation to a flow signal from a pneumotach.
Contents
Introduction
Overview
Scope
Version History
Method Overview
Normal Breathing
Hypopnea
Central Apneas
Flow Restriction
Discussion
Bibliography
---
Introduction
Overview
In this document we discuss calibrated respiratory inductance plethysmography flow signals (cRIPFlow) and through examples we demonstrate how they compare to actual respiratory flow signals acquired by a calibrated Hans-Rudolph pneumotach.
cRIPFlow signals are derived from RIP measurements of the abdomen and thorax. The measured RIP signals indicate the movement of the abdomen and thorax. By following the movement of the abdomen and thorax over time a flow signal, cRIPFlow, can be derived.
The placement of the RIP belts over the abdomen and thorax can influence the size of each signal with relation to breathing. A calibration of the measured signals is performed to correctly estimate the contribution of the abdomen and thorax to breathing.
A cRIPFlow signal is obtained by measuring the rate of change from the cRIPSum by taking the time derivative
cRIPSum = k*A + T
cRIPFlow = d (cRIPSum)/dt
where A and T are the measured Abdomen and Thorax flow signals, respectively, and kA is the calibration value to be determined by a calibration method. A simple summation of A and T (i.e. kA = 1) is not accurate since the value of kA changes depending on both the placement of the belts on the body and the shape of the patient. An accurate value of kA is therefore needed if the cRIPFlow signal is to represent the actual flow. Calibrated RIP belts are discussed in more detail in [1].
An older method used to estimate flow from the RIP measurements is RIPFlow. This method uses a measure of the phase difference of the Abdomen and Thorax movements to modulate the flow amplitude. This resulted in flow traces where apnea and hypopnea like traces were produced artificially due to the modulation. This problem has been solved in the cRIPFlow.
Scope
We use plots to compare Noxturnal calibrated RIP flow, cRIPFlow, to a flow signal acquired by a calibrated Hans-Rudolph pneumotach. Furthermore, we show how an older approach to calculating flow based on the RIP signal, RIPFlow, can produce an overestimate of hypopneas and apneas. The figures show how the cRIPFlow and RIPFlow correspond to the pneumotach flow signal under different circumstances during sleep.
Version History
Method Overview
The following figures show the difference between the RIP flow signals to the pneumotach device, Hans Rudolph. The figures show the trace representing the flow measured by: the Hans Rudolph pneumotach, the cRIPFlow, the RIPFlow, and the movement of the Abdomen and Thorax. No filtering schemes are applied.
To quantify the similarities between the calibrated signal and Hans Rudolph we use the Pearson product-moment correlation coefficient.
Devices: T3 and pneumotach device Hans Rudolph
Software: Matlab r2012
Normal Breathing
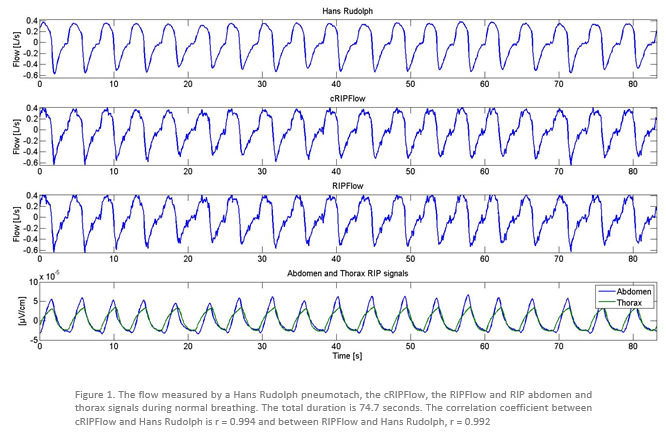
The most noticeable difference between the two RIP flow signals and the pneumotach Hans Rudolph is that they are not as smooth as Hans Rudolph. This spurious effect is attributed to the heart which is picked up in the RIP belts. A detailed discussion of this heart artifact in RIP belts can be found in [2].
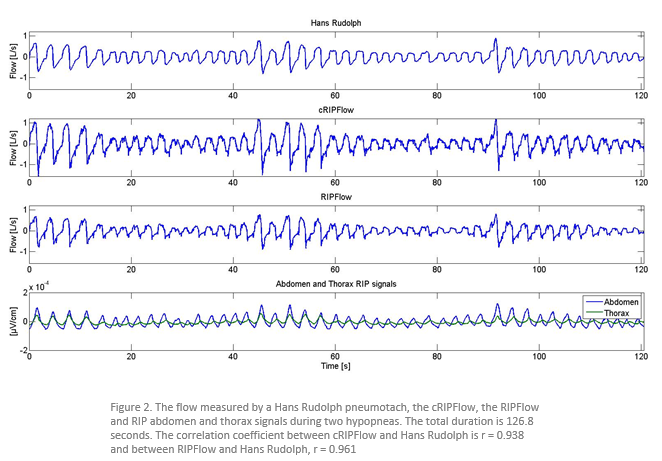
Hypopnea
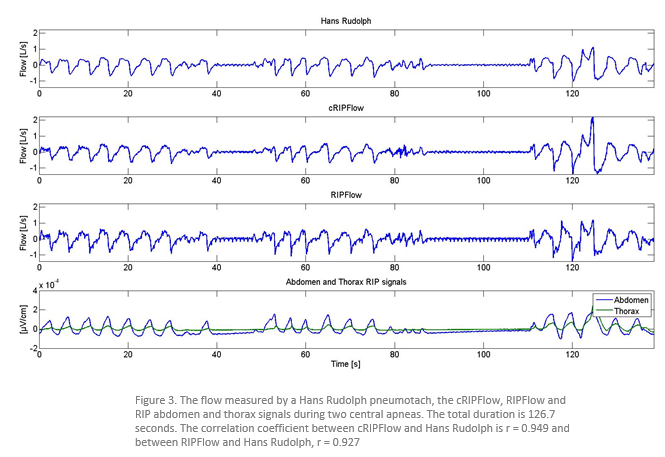
Central Apneas
Flow Restriction
Discussion
The comparison show a high correlation between the flow measured by a Hans Rudolph pneumotach and the cRIPFlow measured by the RIP belts. The correlation coefficient is larger than r = 0.940 in all of the examples.
The cRIPFlow can be used to distinguish between normal breathing, hypopneas, and central apneas as a pneumotach flow measurement.
The cRIPFlow uses a patented automatic real time calibration method developed by Nox Medical.
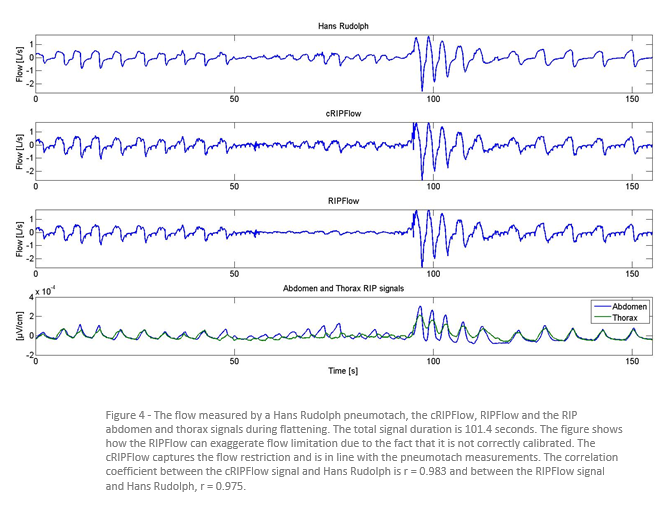
The cRIPFlow captures the breathing pattern accurately compared to the Hans Rudolph pneumotach while the RIPFlow is shown to exaggerate flow limitation in some cases, such as in Figure 4.
The heart beating is known to influence the RIP measurements. This does not reduce the usefulness of the method, although some details in the flow may be masked by the heart signal.
In the paper the cRIPFlows were calibrated to show the flow in liters per second. This calibration was performed to make it easier for the reader to compare the two signals. This calibration does not influence the measured correlation coefficients.
No obstructive apneas occurred in the test measurements.
The measurements were carried out on 20 individuals from a normal population.
Bibliography
[1] RIP Technology and Flow
http://support.noxmedical.com/
S. Hoskuldsson, H.T. Hallgrimsson, and GT Sigurdarson. Method, apparatus, and system for
measuring respiratory effort, PCT/IB2014/002760, November 2014,
[2] (2015-021) Research Darwin - ECG artifacts on RIP flow and cRIP flow
Ver 2.0
Comments